What is it?
A robot assisted laparoscopic partial nephrectomy is using keyhole surgery to remove part of one of your kidneys with the Davinci Robotic surgery system
Why does this need to be done?
You have two kidneys which produce your urine. One of these has a tumour and your surgeon has determined this needs to be removed. After the operation your body should function just as well regarding urine production as before.
Why do I need the nephrectomy performed laparoscopically?
The kidneys lie deep in the back just in front of the lower ribs. The traditional method of performing this operation because of their position requires large incisions at the back or the front of the abdomen. Your surgeon has chosen to remove your kidneys with keyhole surgery in order to minimise the trauma to you. This should reduce the length of recovery, the risk of complications, the postoperative discomfort and allow you to resume your normal life in a shorter period of time compared to the open method. Using the DaVinci robot allows us to perform a more precise excision of the tumour and subsequent suturing of the kidney defect. This reduces the risks of retained cancer, postoperative complications and improves kidney function
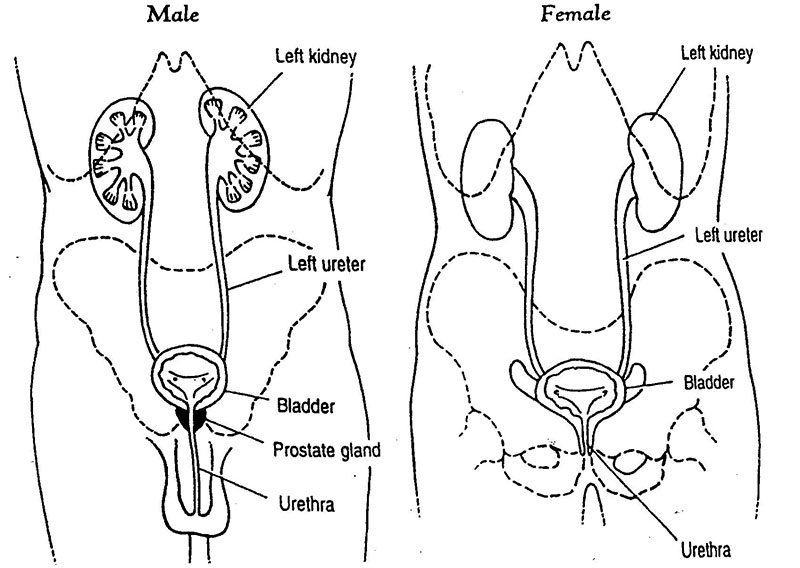
Basic Anatomy
What preparations are needed prior to surgery?
A number of preoperative blood tests will be performed sometimes up to two weeks before the operation and in other circumstances these checks may be done the day before surgery. Time of your admission to hospital will be given to you by the surgical team. You will be given instructions of when the last time you can drink prior to the operation but the general rule is nothing must be taken orally for six hours before the operation.
How is the operation performed?
The operation is performed under general anaesthetic (you will be asleep),and usually tales 2-3 hours. You will lie on your side for all of the operation with a breathing tube through your mouth. The surgeon will make three small stab wounds in your abdomen. Depending on the region of the disease this will either be at the front of the abdomen or in the flank (in the side below your ribs). Occasionally a fourth stab wound will be required. Through one of these stab incisions a laparoscopic camera will be inserted to see inside the abdomen, the kidney and surrounding organs. Through the others, instruments will be inserted to allow the fat surrounding the kidney to be removed and the edges of the tumour identified. The artery to the kidney will be temporarily clamped and the tumour excised from the kidney using laparoscopic scissors. The bleeding edge of the kidney will then be stitched with the laparoscopic instruments and a surgical glue applied to the raw area to prevent bleeding postoperatively. The tumour will then be scooped up through a small bag inserted through one of the wounds{see pictures below}. The bag is then extracted through that wound and the specimen then sent for analysis and examination under the microscope in the laboratory.
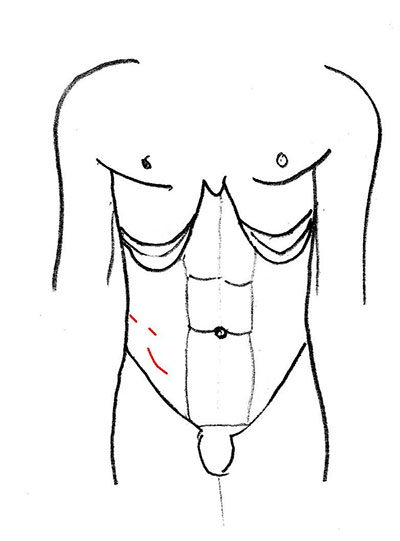
title = incisions expected from flank approach
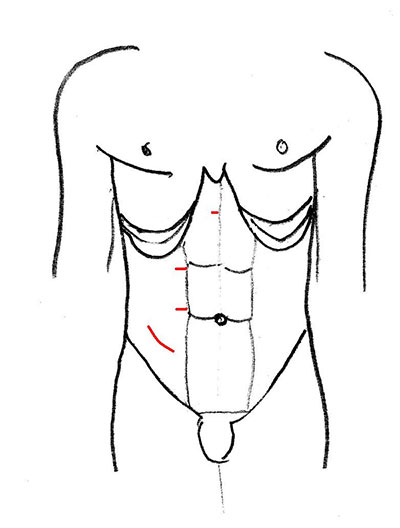
title = incisions expected from front approach
What happens after the operation?
After the operation you will be taken to a recovery ward and following that you will be transferred to a normal ward. You will have a catheter in your bladder. This is a soft plastic tube which drains the urine from the bladder into a bag which hangs beside your bed. The catheter is kept in place by a small balloon inside the bladder which stops the catheter falling out and allows you to move around more freely. You may have a mask on providing oxygen and you will have a fine plastic tube (drip) into your arm which will allow fluids to go into your veins to keep you hydrated until you are eating and drinking normally. You will have a fine plastic tube coming out of your skin wound and occasionally a fine tube (naso gastric) coming out of your nose to allow drainage of wind from your stomach.
Will it hurt?
The wound may be painful and patients may have one of two types of administration of a continuous painkiller that may be required for up to 48hours post surgery. One is called a PCA ( patient.controlled analgesia). This is via a small drip into the arm that allows continuous infusion of painkiller and the patient has a hand button that they are able to press to increase the amount of the painkiller that is inserted via the pump as required. Other patients may have an epidural which is small plastic tube going into the back to administer a continuous drip of painkilling medication. As well as these two methods the patient will be given options of oral and intra-muscle injections of painkillers postoperatively as they require following discussion with the nursing staff. The type of continuous painkilling medication will be discussed with you by the anaesthetist prior to the operation. If an epidural (tube into the back) is required it will be inserted prior to the operation commencing. By 48 hours post surgery most of the patients require no continuous method of painkillers, requiring simply occasional oral medication.
Drinking and eating
Patients may feel sick for up to 24 hours postoperatively but this usually is transient and medication can be given to alleviate this. The majority of patients will start drinking within 24 hours after the operation often taking light diet leading up to commencement of full diet within 48 hours.
Opening bowels?
It is quite normal for bowels not to be open for a number of days post surgery. Passing wind usually takes 48 to 72 hours and passing a formed stool may be longer than this. If this is uncomfortable laxatives can be given but in general patients do not have their hospital discharge delayed by the need to have their bowels open.
Passing urine?
The catheter in the bladder may be in place for a day or two and is usually removed after 24 hours on the ward and removal of this is a procedure requiring no covering pain killers but is usually performed after administering antibiotic into the arm.
The wound
The wound will have dressings which may show some staining with old blood in the first 24 hours. It is possible to see some bruising in the skin around the wound after 48 hours. The majority of wounds will be adhered together with stitches in the muscle under the skin and small clips in the skin itself. The small metal clips will be removed by the district nurse approximately 10 days after the operation. The skin drain that was inserted at the time of the operation is usually removed within 48 hours.
Prophylactic treatment?
In order to reduce the risk of wound infection the anaesthetist will administer intravenous antibiotics at the time of the operation. In order to reduce the risk of thrombosis in the legs, stockings will be worn by patients at the time of the operation until discharge and a small injection of blood thinning medication will be given into the stomach on an early basis.
Washing
The area around the wound can be washed as soon as the dressing has been removed and shower are entirely appropriate 48hours following surgery despite having different tubes coming from the body.
How long will I be in hospital?
Patients should plan to be in hospital for three days post surgery although occasionally patients do take a little longer. An appointment will be made for you on discharge to be seen by the surgeon either 2 to 6 weeks post surgery.
After I leave hospital - general advice
You are likely to feel quite tired for a month following surgery. You will be gradually improving during this time although you will begin to physically perform tasks that you did prior to surgery within a week without risk of damage to you or the wounds. You will find that these will tire you more than usual. Aches and twinges in the wound can be felt for a number of weeks post surgery. You will be able to drive as soon as you can make an emergency stop without discomfort in the wound which is normally approximately a week following surgery and you can start a sexual relationship when the wound feels more comfortable.
What are the possible complications?
There is a 1% chance that during the surgery difficulties will be encountered preventing Laparoscopic partial nephrectomy. The options would be to proceed to Laparoscopic full nephrectomy or conversion to an open incision to perform the partial nephrectomy. Your surgeon will discuss with you in advance this scenario to guide the cause of action in these circumstances.
Minor chest inflammation requiring breathing exercises is commonly seen but major infections requiring antibiotics occur in under 2%. Haemorrhage may necessitate blood transfusion in 5% of cases. Return to theatre to deal with complications is seen in 2% of cases. Infection at the wound site is seen in under 2% of cases and hernia of the incision site is a rare complication in less than 1 in 500 Other complications are increasingly rare which includes injury to nearby organs or blood vessels or entry into the lung cavity.